You might also like
- Laboratory Tests and Diagnostic Procedures, 6E (2013) (UnitedVRG) PDFDocument1,235 pagesLaboratory Tests and Diagnostic Procedures, 6E (2013) (UnitedVRG) PDFrisovi100% (7)
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- Cardiac MarkersDocument23 pagesCardiac MarkersAsmaaYLNo ratings yet
- Oncology Lectures 1 7 DR - FerrolinoDocument24 pagesOncology Lectures 1 7 DR - FerrolinoMiguel Cuevas DolotNo ratings yet
- Renal Cell Carcinoma Risk Factors & TypesDocument1 pageRenal Cell Carcinoma Risk Factors & TypesBobet ReñaNo ratings yet
- Acute Coronary Syndrome: Dr. H.M. Saifullah Napu, SPJP, FihaDocument47 pagesAcute Coronary Syndrome: Dr. H.M. Saifullah Napu, SPJP, FihaJual Beli Promosi100% (1)
- Anemia PDFDocument36 pagesAnemia PDFJANo ratings yet
- Cerebrovascular Accident (CVA)Document71 pagesCerebrovascular Accident (CVA)nur muizzah afifah hussinNo ratings yet
- Pathophysiology of Ischemic Stroke FinalDocument3 pagesPathophysiology of Ischemic Stroke FinalAcohCChao67% (3)
- Neck Trauma LecDocument49 pagesNeck Trauma Lecapi-3743483100% (2)
- 2017 Master Hematology and Coagulation Checklist CAPDocument84 pages2017 Master Hematology and Coagulation Checklist CAPJo San JuanNo ratings yet
- Baranova ResumeDocument2 pagesBaranova Resumeapi-252948975No ratings yet
- 13.24 Abdominal-InjuryDocument42 pages13.24 Abdominal-InjuryMuhammad FajarNo ratings yet
- Drug AbuseDocument5 pagesDrug AbuseSajeel ZamanNo ratings yet
- Concept Map 3 MM (Abdominal Pain)Document2 pagesConcept Map 3 MM (Abdominal Pain)Matt McKinleyNo ratings yet
- Heart Disease in Pregnancy: Mohana PreeshaDocument50 pagesHeart Disease in Pregnancy: Mohana PreeshaChuks LeviNo ratings yet
- Fluid Resuscitation and Organ Perfusion EvaluationDocument66 pagesFluid Resuscitation and Organ Perfusion EvaluationDewiRatnasariNo ratings yet
- Cardiac Biomarker PresentationDocument29 pagesCardiac Biomarker PresentationMohana PreeshaNo ratings yet
- Principles of OcclusionDocument73 pagesPrinciples of OcclusionbkprosthoNo ratings yet
- Hodgkin LymphomaDocument44 pagesHodgkin LymphomaisnineNo ratings yet
- Principles of OncologyDocument26 pagesPrinciples of OncologyDr Shahzad Alam ShahNo ratings yet
- Effect of hemodialysis on selected drugsDocument3 pagesEffect of hemodialysis on selected drugsHannah Angelica RemoNo ratings yet
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocument38 pagesAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasNo ratings yet
- Tan NotesDocument26 pagesTan NotesVishal Yogi100% (6)
- Manage StrokeDocument35 pagesManage StrokeAisyah IcahNo ratings yet
- TPNDocument69 pagesTPNMylz MendozaNo ratings yet
- 7 Liver - Spleen TraumaDocument34 pages7 Liver - Spleen Traumabagus75% (4)
- A Survey of Oncology Advanced Practice Nurses in Ontario: Profile and Predictors of Job SatisfactionDocument19 pagesA Survey of Oncology Advanced Practice Nurses in Ontario: Profile and Predictors of Job SatisfactionNYONGKERNo ratings yet
- Cardiac BiomarkersDocument72 pagesCardiac BiomarkersAmey JatharNo ratings yet
- Everything You Need to Know About Surveyors and Surveying in Removable Partial DenturesDocument82 pagesEverything You Need to Know About Surveyors and Surveying in Removable Partial DenturesKelly Yeow50% (2)
- Bone Marrow BiopsyDocument28 pagesBone Marrow BiopsyAmeer MattaNo ratings yet
- Tumor marker classification and applicationsDocument30 pagesTumor marker classification and applicationsnouval_iqbal100% (1)
- Cardiac Output FactorsDocument61 pagesCardiac Output FactorsSyed Ali MoosaNo ratings yet
- Management of Heart FailureDocument62 pagesManagement of Heart Failureapi-13265958No ratings yet
- Cholangiocarcinoma: The Right Clinical Information, Right Where It's NeededDocument40 pagesCholangiocarcinoma: The Right Clinical Information, Right Where It's NeededHan KethyanethNo ratings yet
- Thoracic Injury Management Jan 08Document39 pagesThoracic Injury Management Jan 08Uday PrabhuNo ratings yet
- Principles of Oncology NursingDocument12 pagesPrinciples of Oncology NursingДария Коваленко100% (1)
- Infection Control BasicsDocument10 pagesInfection Control BasicsAlan Amato100% (1)
- Principle of ElectroDx by Dr. Angkana Nudsasarn, Chiang Mai UniversityDocument113 pagesPrinciple of ElectroDx by Dr. Angkana Nudsasarn, Chiang Mai UniversitySurat Tanprawate100% (3)
- Liver Cirrhosis: Causes, Complications and ManagementDocument55 pagesLiver Cirrhosis: Causes, Complications and ManagementAnonymous vUEDx8100% (1)
- Evaluation of Chest Pain: Ruling Out Life ThreatsDocument16 pagesEvaluation of Chest Pain: Ruling Out Life ThreatsAbhinit RiddhiNo ratings yet
- Cardiac MarkerDocument19 pagesCardiac MarkersriworoNo ratings yet
- Coronary Artery Disease: Causes, Risks, and PreventionDocument80 pagesCoronary Artery Disease: Causes, Risks, and Preventionamelia pratiwiNo ratings yet
- Non-Variceal Upper GI Bleeding GuideDocument34 pagesNon-Variceal Upper GI Bleeding GuideChe Ainil ZainodinNo ratings yet
- CBC interpretation guideDocument37 pagesCBC interpretation guideMusleh Al MusalhiNo ratings yet
- RBC Degradation & Causes of JaundiceDocument30 pagesRBC Degradation & Causes of JaundiceSubhi MishraNo ratings yet
- Acute Necrotizing PancreatitisDocument37 pagesAcute Necrotizing PancreatitisVania SuSanchezNo ratings yet
- Approach To Thyroid NoduleDocument33 pagesApproach To Thyroid Nodulerajan kumar100% (5)
- CANCER History of Cancer Chemotherapy 2008Document12 pagesCANCER History of Cancer Chemotherapy 2008gustavopsoNo ratings yet
- Laboratory Values of Clinical ImportanceDocument46 pagesLaboratory Values of Clinical ImportanceIndrajit Rana100% (3)
- Nursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalDocument55 pagesNursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalFayizatul AkmarNo ratings yet
- RN GI Endoscopy, Operating RoomDocument4 pagesRN GI Endoscopy, Operating Roomapi-78554516100% (1)
- Clinical Practice Guideline For CataractDocument27 pagesClinical Practice Guideline For CataractNaufal FarisatriantoNo ratings yet
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- Febrile Neutropenia: Nontapak ThiangpakDocument53 pagesFebrile Neutropenia: Nontapak ThiangpakRapid MedicineNo ratings yet
- Metabolic Response to Trauma: Understanding the Physiological ConsequencesDocument52 pagesMetabolic Response to Trauma: Understanding the Physiological ConsequencesAnil BasnetNo ratings yet
- 2 Acute Myocardial InfarctionDocument15 pages2 Acute Myocardial InfarctionpauchanmnlNo ratings yet
- Pediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIDocument27 pagesPediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIAfied Fitrah100% (1)
- Thyroid CancerDocument15 pagesThyroid CancerA. Lizette PabloNo ratings yet
- Regulation of calcium, Parathyroid hormone, Vitamin D & CalcitoninDocument29 pagesRegulation of calcium, Parathyroid hormone, Vitamin D & CalcitoninJessica StewartNo ratings yet
- CT and MRI of Abdomen and PelvicDocument1,691 pagesCT and MRI of Abdomen and PelvicĐức Khang NguyễnNo ratings yet
- Critical Care in PregnancyDocument21 pagesCritical Care in PregnancyamuzaNo ratings yet
- Renal Physiology 1Document9 pagesRenal Physiology 1Anny AlvrzNo ratings yet
- Crp-DikonversiDocument13 pagesCrp-DikonversiKurnia FitriasariNo ratings yet
- Approach to Hypertension ManagementDocument11 pagesApproach to Hypertension ManagementNoreenNo ratings yet
- Basic Principles of PharmacologyDocument34 pagesBasic Principles of Pharmacologyrabia khalidNo ratings yet
- CardiacDocument37 pagesCardiacmeghanaNo ratings yet
- Biomarkers for diagnosing acute myocardial infarctionDocument7 pagesBiomarkers for diagnosing acute myocardial infarctionBryan GarmaNo ratings yet
- O2 ThearpyDocument6 pagesO2 ThearpyKelly YeowNo ratings yet
- ParaprteinemiaDocument32 pagesParaprteinemiaKelly YeowNo ratings yet
- Major Histocompatibility Complex 12032018Document39 pagesMajor Histocompatibility Complex 12032018Kelly YeowNo ratings yet
- Lymphadenopathy LymphomaDocument72 pagesLymphadenopathy LymphomaKelly YeowNo ratings yet
- HIV Infections and AIDSDocument42 pagesHIV Infections and AIDSKelly YeowNo ratings yet
- Blood Transfusion Reaction 3032018Document33 pagesBlood Transfusion Reaction 3032018Kelly YeowNo ratings yet
- PneumoniaDocument34 pagesPneumoniaKelly YeowNo ratings yet
- OBSTRUCTIVE PULMONARY DISEASE - COPD-revisedDocument49 pagesOBSTRUCTIVE PULMONARY DISEASE - COPD-revisedKelly YeowNo ratings yet
- OBSTRUCTIVE PULMONARY DISEASE - COPD-revisedDocument49 pagesOBSTRUCTIVE PULMONARY DISEASE - COPD-revisedKelly YeowNo ratings yet
- TuberculosisDocument45 pagesTuberculosisKelly YeowNo ratings yet
- TuberculosisDocument45 pagesTuberculosisKelly YeowNo ratings yet
- Blood Transfusion Reaction 3032018Document33 pagesBlood Transfusion Reaction 3032018Kelly YeowNo ratings yet
- HIV Infections and AIDSDocument42 pagesHIV Infections and AIDSKelly YeowNo ratings yet
- Lymphadenopathy LymphomaDocument72 pagesLymphadenopathy LymphomaKelly YeowNo ratings yet
- Principles of Chemotherapy DR VetriDocument28 pagesPrinciples of Chemotherapy DR VetriKelly YeowNo ratings yet
- ZddBI0 36 Management of A MaxillaryDocument5 pagesZddBI0 36 Management of A MaxillaryKelly YeowNo ratings yet
- Major Histocompatibility Complex 12032018Document39 pagesMajor Histocompatibility Complex 12032018Kelly YeowNo ratings yet
- Viral Hepatitis-DDS 2 - 2017-18Document48 pagesViral Hepatitis-DDS 2 - 2017-18Kelly YeowNo ratings yet
- Lymphadenopathy LymphomaDocument72 pagesLymphadenopathy LymphomaKelly YeowNo ratings yet
- A Clinical Guide To Endodontics - Update Part 2Document8 pagesA Clinical Guide To Endodontics - Update Part 2Kelly YeowNo ratings yet
- AirwaysDocument2 pagesAirwaysLestari Chye PouedanNo ratings yet
- Abdomen AgudoDocument8 pagesAbdomen AgudoELizabeth OlmosNo ratings yet
- Negotiating Double CurvatureDocument5 pagesNegotiating Double CurvatureAnonymous HQtjVBrPNo ratings yet
- Endodontic Management of Aberrant Root C PDFDocument4 pagesEndodontic Management of Aberrant Root C PDFKelly YeowNo ratings yet
- Psychological Development DomainsDocument3 pagesPsychological Development DomainsKelly Yeow100% (1)
- Cbnicalertsalivainsert 170113213726Document2 pagesCbnicalertsalivainsert 170113213726Kelly YeowNo ratings yet
- Flow DiagramDocument45 pagesFlow DiagramKelly YeowNo ratings yet
- Cbnicalertsalivainsert 170113213726Document2 pagesCbnicalertsalivainsert 170113213726Kelly YeowNo ratings yet
- Cefixime oral suspension SPC summaryDocument9 pagesCefixime oral suspension SPC summaryPharmacist ipsNo ratings yet
- Stress ProjectDocument21 pagesStress ProjectaisyahambaliNo ratings yet
- Heart Disease in PregnancyDocument5 pagesHeart Disease in PregnancyAngeliqueNo ratings yet
- Impact BariatricDocument8 pagesImpact BariatricHar YudhaNo ratings yet
- Patient's Profile: Doña Remedios Trinidad Romualdez Medical Foundation, Inc. 2 Semester, S.Y. 2020-2021Document16 pagesPatient's Profile: Doña Remedios Trinidad Romualdez Medical Foundation, Inc. 2 Semester, S.Y. 2020-2021Royce Vincent TizonNo ratings yet
- Gallstones: Mitchell Conn Educational GoalsDocument8 pagesGallstones: Mitchell Conn Educational GoalsIan Evan LeeNo ratings yet
- Bethel Schools 2018-2019 CalendarDocument1 pageBethel Schools 2018-2019 CalendarSinclair Broadcast Group - EugeneNo ratings yet
- EmpyemaDocument33 pagesEmpyemavirz23100% (1)
- Exploring School Nurse Interventions and Health and Education Outcomes: An Integrative ReviewDocument14 pagesExploring School Nurse Interventions and Health and Education Outcomes: An Integrative ReviewpaoNo ratings yet
- Ayurvision 09 e BookDocument75 pagesAyurvision 09 e BookCesar Aguilar100% (1)
- Medication Template BaclofenDocument2 pagesMedication Template BaclofenJudith MeranvilNo ratings yet
- Fitness PowerpointDocument42 pagesFitness PowerpointKellie GuestNo ratings yet
- Mental Health PresentationDocument29 pagesMental Health Presentationwambundegwa99No ratings yet
- Major Risk Factors for Cardiovascular DiseasesDocument28 pagesMajor Risk Factors for Cardiovascular DiseasesMannat ZaidiNo ratings yet
- Health QuizDocument6 pagesHealth QuizBrith FranklinNo ratings yet
- Reforms Corresponding To The Population Ageing: The Case of JapanDocument22 pagesReforms Corresponding To The Population Ageing: The Case of JapanADBI EventsNo ratings yet
- Pasteurisation Dairy-Science ResearchDocument62 pagesPasteurisation Dairy-Science ResearchRavi Chandran RNo ratings yet
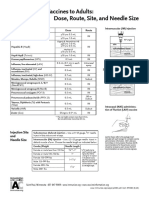
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashNo ratings yet
- Outbreaks Where Food Workers Have Been Implicated in The Spread of Foodborne Disease. Part 6. Transmission and Survival of Pathogens in The Food Processing and Preparation EnvironmentDocument18 pagesOutbreaks Where Food Workers Have Been Implicated in The Spread of Foodborne Disease. Part 6. Transmission and Survival of Pathogens in The Food Processing and Preparation EnvironmentCalidad CODITEV SACNo ratings yet
- Artikel Nama Medis DhionDocument2 pagesArtikel Nama Medis DhionDhion HernandoNo ratings yet
- Sports PhysicalDocument4 pagesSports Physicalapi-209628543No ratings yet
- Disc Edema Ento KeyDocument2 pagesDisc Edema Ento KeyumakantsinghNo ratings yet
- Tick-Borne Diseases in Turkey A Review One Health ApproachDocument12 pagesTick-Borne Diseases in Turkey A Review One Health ApproachAamir muse osmanNo ratings yet