You might also like
- Bob Jones - Science 4Document254 pagesBob Jones - Science 4kage_urufu100% (4)
- Phantom Susan KayDocument379 pagesPhantom Susan Kaytheeyeofthemoon100% (9)
- Web Search - One People's Public Trust 1776 UCCDocument28 pagesWeb Search - One People's Public Trust 1776 UCCVincent J. CataldiNo ratings yet
- Why Narcissists Need You To Feel Bad About Yourself - Psychology TodayDocument51 pagesWhy Narcissists Need You To Feel Bad About Yourself - Psychology Todaytigerlo75No ratings yet
- Liquid Hydrogen As A Propulsion Fuel, 1945-1959Document341 pagesLiquid Hydrogen As A Propulsion Fuel, 1945-1959Bob AndrepontNo ratings yet
- ACLSDocument39 pagesACLSJason LiandoNo ratings yet
- Cardiac CatheterizationDocument9 pagesCardiac CatheterizationAnurag Gupta100% (1)
- Handout of English For PsychologyDocument75 pagesHandout of English For PsychologyRivan Dwi AriantoNo ratings yet
- Adult Advanced Life Support GuidelinesDocument11 pagesAdult Advanced Life Support GuidelinesRuvan AmarasingheNo ratings yet
- Onsemi ATX PSU DesignDocument37 pagesOnsemi ATX PSU Designusuariojuan100% (1)
- DirtyMobs' Ultimate Matchup GuideDocument5 pagesDirtyMobs' Ultimate Matchup GuideTempest JannaNo ratings yet
- Swarthz TRAUMADocument26 pagesSwarthz TRAUMAAlexandra Niken Larasati75% (4)
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
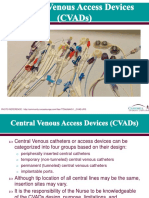
- Central Venous AccessDocument20 pagesCentral Venous AccessCarlos GuerreroNo ratings yet
- Cabg NursingDocument7 pagesCabg NursingDennis Cobb100% (1)
- 09 ITLS PretestDocument6 pages09 ITLS PretestArlanosaurus100% (2)
- 09 ITLS PretestDocument6 pages09 ITLS PretestArlanosaurus100% (2)
- Perioperative Care For CABG PatientsDocument32 pagesPerioperative Care For CABG PatientsAya EyadNo ratings yet
- The Art of Woodworking Shaker FurnitureDocument147 pagesThe Art of Woodworking Shaker Furnituremalefikus100% (2)
- CPR PDFDocument37 pagesCPR PDFArdhi AgustjikNo ratings yet
- Trauma and Emergency NursingDocument9 pagesTrauma and Emergency Nursingchinthaka18389021No ratings yet
- Evelyn Nakano Glenn, "From Servitude To Service Work: Historical Continuities in The Racial Division of Paid Reproductive Labor"Document44 pagesEvelyn Nakano Glenn, "From Servitude To Service Work: Historical Continuities in The Racial Division of Paid Reproductive Labor"s0metim3sNo ratings yet
- Caring For A Patient After Coronary Artery Bypass.6Document6 pagesCaring For A Patient After Coronary Artery Bypass.6Nadia BeadleNo ratings yet
- A Study On Inventory Management Towards Organizational Performance of Manufacturing Company in MelakaDocument12 pagesA Study On Inventory Management Towards Organizational Performance of Manufacturing Company in MelakaOsama MazharNo ratings yet
- Cateter Venoso Central PDFDocument37 pagesCateter Venoso Central PDFClaris PachecoNo ratings yet
- Anzcor Guideline 11 10 1 Als Traumatic Arrest 27apr16Document11 pagesAnzcor Guideline 11 10 1 Als Traumatic Arrest 27apr16Mario Colville SolarNo ratings yet
- ATLS 8th Edition Update,: By: Fatma Al-GhaithiDocument37 pagesATLS 8th Edition Update,: By: Fatma Al-GhaithiJustin Salazar VenegasNo ratings yet
- Central Venous PressureDocument4 pagesCentral Venous Pressuremike_steven12No ratings yet
- CathSap BDocument153 pagesCathSap BSajjad HussainNo ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Acute/Critically Ill Patients in Hemodynamic Monitoring (Management)Document8 pagesAcute/Critically Ill Patients in Hemodynamic Monitoring (Management)Esmareldah Henry SirueNo ratings yet
- Politrauma - Rolul AtiDocument18 pagesPolitrauma - Rolul AtiChirita ElenaNo ratings yet
- CANULADocument12 pagesCANULAAlejandro Salazar TorresNo ratings yet
- Pleural Procedures in Critically Ill PatientsDocument9 pagesPleural Procedures in Critically Ill PatientsFlávio VillaNo ratings yet
- The FourDocument22 pagesThe FourInatul AuliaNo ratings yet
- Quality Guidelines IVC FilterDocument9 pagesQuality Guidelines IVC Filteramrit koiralaNo ratings yet
- Arteri LineDocument13 pagesArteri Linemuthia octavianaNo ratings yet
- Adult Advanced Life Support GuidelinesDocument11 pagesAdult Advanced Life Support GuidelinesDellaneira SetjiadiNo ratings yet
- Adult Advanced Life Support GuidelinesDocument11 pagesAdult Advanced Life Support Guidelinesrutba.ahmkhanNo ratings yet
- CVPDocument25 pagesCVPNikhil YadavNo ratings yet
- Pediatric Vascular Access SelectionDocument16 pagesPediatric Vascular Access SelectionNatascha CabralNo ratings yet
- A Critical Care Echocardiography-Driven Approach To Undifferentiated ShockDocument7 pagesA Critical Care Echocardiography-Driven Approach To Undifferentiated ShockNoel Saúl Argüello SánchezNo ratings yet
- Traum ManagementDocument7 pagesTraum Managementchinthaka18389021No ratings yet
- Journal Reading BTS Guidelines For The Management of Spontaneous PneumothoraxDocument42 pagesJournal Reading BTS Guidelines For The Management of Spontaneous PneumothoraxDhyan KidiNo ratings yet
- CPR: Essentials of Cardiopulmonary ResuscitationDocument7 pagesCPR: Essentials of Cardiopulmonary Resuscitationdaniphilip777No ratings yet
- Jurnal ReadingDocument22 pagesJurnal ReadingSherin Adha HadiaNo ratings yet
- 3-Monitoreo Del PX en EmergenciasDocument6 pages3-Monitoreo Del PX en EmergenciasHoracio A. AguilarNo ratings yet
- (FEU) Central Venous Pressure Notes PDFDocument25 pages(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNo ratings yet
- Central Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesDocument26 pagesCentral Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesShofarie AhmadNo ratings yet
- Clinical Management of The Extracorporeal Membrane Oxygenation CircuitDocument7 pagesClinical Management of The Extracorporeal Membrane Oxygenation CircuitRicardoNo ratings yet
- Ultrasound Guided Percutaneous DrainageDocument3 pagesUltrasound Guided Percutaneous DrainageLaraib Fatima0% (1)
- Vein - 2009 Sir - Ivcf ReviewDocument9 pagesVein - 2009 Sir - Ivcf Reviewjohn_smith_532No ratings yet
- ct- cardiac tamponade 2013Document5 pagesct- cardiac tamponade 2013floNo ratings yet
- CVC Partner 1Document40 pagesCVC Partner 1stefani83No ratings yet
- AtlsDocument34 pagesAtlsmagesa.lazaroNo ratings yet
- Intervencion Usg EmergenciasDocument22 pagesIntervencion Usg EmergenciasSaul Gonzalez HernandezNo ratings yet
- Central Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesDocument22 pagesCentral Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesNenazNaziahNo ratings yet
- RACE 2017 MegacodeDocument33 pagesRACE 2017 MegacodemickeyNo ratings yet
- Ivc FilterDocument15 pagesIvc FilterashishNo ratings yet
- Central Venous PreasureDocument22 pagesCentral Venous PreasureD ZamiatNo ratings yet
- Pulmonary Function Tests and Lung ResectionDocument9 pagesPulmonary Function Tests and Lung ResectionPrabhakar KumarNo ratings yet
- Cardiac ArrestDocument30 pagesCardiac ArrestagnescheruseryNo ratings yet
- Eco DopplerDocument8 pagesEco DopplerClaudia IsabelNo ratings yet
- 2 150507152224 Lva1 App6892Document55 pages2 150507152224 Lva1 App6892poojaNo ratings yet
- Management of Spontaneous PneumothoraxDocument45 pagesManagement of Spontaneous Pneumothoraxbanjar1982No ratings yet
- Clinical Review: Hemodynamic Monitoring in The Intensive Care UnitDocument8 pagesClinical Review: Hemodynamic Monitoring in The Intensive Care Unitmasfak97No ratings yet
- Chest Wall, Lung, Mediastinum, and Pleura ProceduresDocument124 pagesChest Wall, Lung, Mediastinum, and Pleura ProceduresKenn BrillanteNo ratings yet
- 56 Anaesthesia For Carotid Endarterectomy PDFDocument10 pages56 Anaesthesia For Carotid Endarterectomy PDFHarish BhatNo ratings yet
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDocument6 pagesTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142No ratings yet
- Diagnostic Evaluation in Respiratory Conditions-1Document68 pagesDiagnostic Evaluation in Respiratory Conditions-1pashiem88No ratings yet
- The Spleen: Splenic Trauma and Splenectomy: TrunkDocument3 pagesThe Spleen: Splenic Trauma and Splenectomy: TrunkAsish GeiorgeNo ratings yet
- JTD 13 03 1886Document13 pagesJTD 13 03 1886Nongnapat KettungmunNo ratings yet
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosFrom EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo ratings yet
- Too Many Normal Saline? Fluids in Various ConditionDocument26 pagesToo Many Normal Saline? Fluids in Various ConditionHandrian RahmanNo ratings yet
- Keeping Children With Disabilities Safe in EmergenciesDocument14 pagesKeeping Children With Disabilities Safe in EmergenciesHandrian RahmanNo ratings yet
- Saline Flush TestDocument5 pagesSaline Flush TestHandrian RahmanNo ratings yet
- Practice Guidelines For Central Venous Access PDFDocument35 pagesPractice Guidelines For Central Venous Access PDFJulio AltamiranoNo ratings yet
- US vs CXR for Confirming CVC PlacementDocument6 pagesUS vs CXR for Confirming CVC PlacementHandrian RahmanNo ratings yet
- Central Catheter Position PDFDocument3 pagesCentral Catheter Position PDFLuen HoNo ratings yet
- Central Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and CorrectionDocument7 pagesCentral Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and CorrectionHandrian RahmanNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportHandrian RahmanNo ratings yet
- Vas Opressor GL 2015Document16 pagesVas Opressor GL 2015Paulus SidhartaNo ratings yet
- Practice Guidelines For Central Venous Access PDFDocument35 pagesPractice Guidelines For Central Venous Access PDFJulio AltamiranoNo ratings yet
- Central Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and CorrectionDocument7 pagesCentral Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and CorrectionHandrian RahmanNo ratings yet
- Central Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and CorrectionDocument7 pagesCentral Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and CorrectionHandrian RahmanNo ratings yet
- Pi Is 0300957217302873Document1 pagePi Is 0300957217302873Handrian RahmanNo ratings yet
- 1 PBDocument2 pages1 PBHandrian RahmanNo ratings yet
- 2012 ResuscitationDocument5 pages2012 ResuscitationHandrian RahmanNo ratings yet
- Research Article: Factors Affecting The Occurrence of Out-of-Hospital Sudden Cardiac ArrestDocument7 pagesResearch Article: Factors Affecting The Occurrence of Out-of-Hospital Sudden Cardiac ArrestHandrian RahmanNo ratings yet
- European Journal of Internal Medicine: Andjelic Sladjana, Panic Gordana, Sijacki AnaDocument8 pagesEuropean Journal of Internal Medicine: Andjelic Sladjana, Panic Gordana, Sijacki AnaHandrian RahmanNo ratings yet
- Post ROSC SurvivorDocument8 pagesPost ROSC SurvivorsarintiNo ratings yet
- OHCA CaseDocument9 pagesOHCA CaseHandrian RahmanNo ratings yet
- DCR FinalDocument32 pagesDCR FinalHandrian RahmanNo ratings yet
- Echocardiography in Emergency - IanDocument15 pagesEchocardiography in Emergency - IanHandrian RahmanNo ratings yet
- Warning: Learners, Please Complete The Learner Survey (Ucalgary - Ca/Codeblue/Surveys) Before Viewing This PowerpointDocument27 pagesWarning: Learners, Please Complete The Learner Survey (Ucalgary - Ca/Codeblue/Surveys) Before Viewing This PowerpointHandrian RahmanNo ratings yet
- Acitaminophen Toxicity - IANDocument32 pagesAcitaminophen Toxicity - IANHandrian RahmanNo ratings yet
- Abd PainDocument35 pagesAbd PainHandrian RahmanNo ratings yet
- Acute Heart FailureDocument19 pagesAcute Heart FailureHandrian RahmanNo ratings yet
- HyperkalemiaDocument13 pagesHyperkalemiaRaZy Abo RayaNo ratings yet
- Abdominal Injury - IanDocument28 pagesAbdominal Injury - IanHandrian RahmanNo ratings yet
- Ashe v. Swenson, 397 U.S. 436 (1970)Document25 pagesAshe v. Swenson, 397 U.S. 436 (1970)Scribd Government DocsNo ratings yet
- ASSIGNMENTDocument5 pagesASSIGNMENTPanchdev KumarNo ratings yet
- Japanese Tea Cups LessonDocument3 pagesJapanese Tea Cups Lessonapi-525048974No ratings yet
- The BrigadeDocument517 pagesThe Brigadele_chiffre4860100% (3)
- Ais 301w Resume AssignmentDocument3 pagesAis 301w Resume Assignmentapi-532849829No ratings yet
- Method of IstinjaDocument24 pagesMethod of IstinjaIslamic LibraryNo ratings yet
- Forms and Types of Business OrganizationDocument2 pagesForms and Types of Business Organizationjune hetreNo ratings yet
- CQI - Channel Quality Indicator - Ytd2525Document4 pagesCQI - Channel Quality Indicator - Ytd2525TonzayNo ratings yet
- 5 - Econ - Advanced Economic Theory (Eng)Document1 page5 - Econ - Advanced Economic Theory (Eng)David JackNo ratings yet
- Muhammad v. Hall, 10th Cir. (2017)Document12 pagesMuhammad v. Hall, 10th Cir. (2017)Scribd Government DocsNo ratings yet
- Semi-Detailed Lesson Plan Template: Pagsanjan Intergrated National High School 8Document3 pagesSemi-Detailed Lesson Plan Template: Pagsanjan Intergrated National High School 8Mae Ganate RoblesNo ratings yet
- Ariel StoryDocument2 pagesAriel StoryKKN Pasusukan2018No ratings yet
- Chap 4 eDocument22 pagesChap 4 eHira AmeenNo ratings yet
- Viennas Cafe Louvre in The 1920s and 1930Document18 pagesViennas Cafe Louvre in The 1920s and 1930Friso HoeneveldNo ratings yet
- Technical Specifications For The: LAMBDA 950 UV/Vis/NIR and LAMBDA 850 UV/Vis SpectrophotometersDocument4 pagesTechnical Specifications For The: LAMBDA 950 UV/Vis/NIR and LAMBDA 850 UV/Vis SpectrophotometersDiogo GálicoNo ratings yet
- OEO105020 LTE ERAN2.2 Connection Management Feature ISSUE 1.00Document52 pagesOEO105020 LTE ERAN2.2 Connection Management Feature ISSUE 1.00Daniel YulistianNo ratings yet
- TOS and CID FORM-TLE 8 ANIMATIONDocument80 pagesTOS and CID FORM-TLE 8 ANIMATIONAriel AntaboNo ratings yet
- Distance Learning 2016 Telecom AcademyDocument17 pagesDistance Learning 2016 Telecom AcademyDyego FelixNo ratings yet
- Guy GacottDocument4 pagesGuy GacottAly ConcepcionNo ratings yet